




First a quick reminder on the four stages of cancer diagnosis:
Stage 1 - this usually means that a cancer is relatively small and contained within the organ it started in.Stage 2 - this usually means the cancer has not started to spread into surrounding tissue but the tumour is larger than in stage 1. Sometimes stage 2 means that cancer cells have spread into lymph nodes close to the tumour. This depends on the particular type of cancer.
Stage 3 usually means the cancer is larger. It may have started to spread into surrounding tissues and there are cancer cells in the lymph nodes in the area.
Stage 4 means the cancer has spread from where it started to another body organ. This is also called secondary or metastatic cancer.
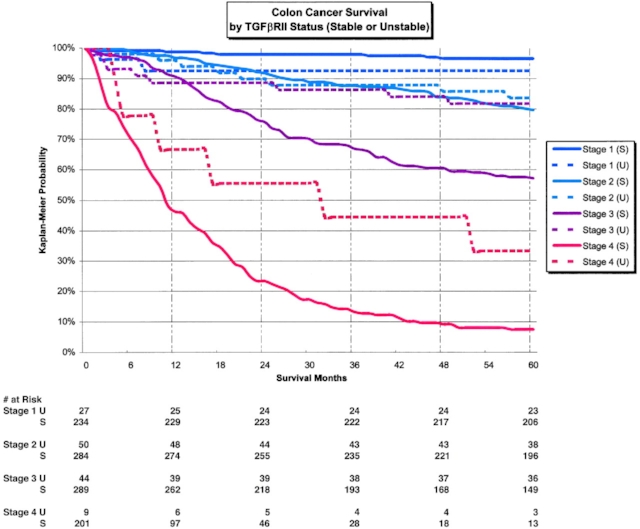
This is very hard to write but it's really important that my family and friends understand this reality. I'm getting a little tired of the "you'll be fine" and "oh my friend had that and he's fine now" emails. Stage 4 mesothelioma is a different ball game because the cancer is deemed to be "metastatic". Not very long ago, a stage 4 colon cancer would be deemed terminal. Today there are odds for survival, but I need you to understand that the official published odds are not good...at all. Survival rates are provided on curves that look like this:

As you can see from this particular study, only 10% of people with my stage 4 diagnosis are alive after 5 years.
Now I am a guy who likes data and I need it to process a situation, and I'll confess that this data scares the crap out of me. However, I've learned that there are several factors that make the interpretation of these medical stats for the purpose of deducing my individual prognosis very problematic.
New innovations - innovation in cancer treatment is proceeding at a rapid pace. For example one of the chemo drugs I'll be on has only recently become available. Therefore these stats, which are generally always at least 5 years old, don't reflect the latest treatment technologies.
I'm not the average bowel cancel patient - Bowel cancer normally hits people much later in life and so the stats are generally based on a very different average patient profile. This is significant because, for example, I'm able to tolerate more aggressive mesothelioma chemotherapy.
Every case is unique - The characteristics of every cancer are unique to each patient. For example, while I'm am technically in stage 4 my liver tumours are very small.
So, how should you think about my prognosis? Well, you should know that the published odds are very bad, but my doctors are encouraging me to think about my odds of surviving this more like a 50/50 bet (I'll talk more about what "survival" of a stage 4 cancer really means in a future post, but think of it simply as being alive in 5 years....not forever).
I've been discussing my personal strategy a lot with my family over the last week. I'll write more about this later but I'm essentially developing a dual track mental model to get through the next few months. On the one hand, I have to be optimistic (studies show your mental attitude has a huge impact on treatment success), but on the other hand, I need to be pragmatic and prepared for the worst, given there is at least a 50% chance of it eventuating. Going down that path of thought is profoundly challenging for a father of three beautiful young children, but I personally think I must go there to get through this.
Stages of Cancer
Staging describes where a cancer is, whether or where it has spread, and whether it affects other parts of the body. Doctors often use diagnostic tests to determine the stage of a cancer. Staging may not be completed until all tests are completed. Knowing the stage helps the doctor:
- Schedule the treatment, including the type of surgery and/or whether chemotherapy or radiotherapy is required
- Predict the likelihood that the cancer will return after the initial treatment
- Prognosis of recovery
- Talk to the entire health team in a clear, common language about the diagnosis
- Determine how well the treatment worked
- Compare how well new treatments work for large groups of people with the same diagnosis
About the TNM staging system
For many cancers, doctors typically use the TNM system of the American Joint Committee on Cancer (AJCC) to describe a stage of cancer. Physicians answer the following questions based on the results of diagnostic tests, imaging scans, and surgeries to remove the tumor or take a sample.
- How big is the primary tumor? Where is it (tumor, T)
- Has the tumor spread to the lymph nodes? If so, where and how many? (Node, N)
- Has the cancer spread to other parts of the body? If so, where and how much? (Metastasis, M)
- Are there any biomarkers or tumor markers associated with the cancer that make it more or less likely to spread?
Staging can be "clinical" or "pathological". Clinical staging is based on the test results that were performed before surgery, eg As in physical examinations and imaging scans. The pathological staging is based on what is found during the operation. The clinical stage is often indicated before the TNM classification with a lowercase letter "c". The pathological stage is indicated by a lowercase letter "p". In general, pathological staging provides the most information to determine a patient's prognosis.
Staging may also be performed after a person has received other treatments before surgery, e.g. As radiotherapy, chemotherapy, hormone therapy or immunotherapy. This is called post-therapy stage. This type of staging can be done for some types of cancer, as a treatment before surgery helps to reduce the size of the tumor so that it can be removed. The post-therapy stage is displayed with a small "y" before the TNM classification.
COMMENTS